Summer Eye Safety
Summertime means spending more time outdoors, at the beach or pool, and more time in the sun. Most people associate more time in the sun with applying sunscreen to protect the skin, but it’s equally as important to protect your eyes, as exposure to harmful sunlight can lead in an increased risk for eye diseases, including cataract, growths on the eye, and even cancer.
In addition to benefitting your vision health, taking precautionary measures to protect your eyes can also make summertime more fun. Follow these simple tips from Georgia Eye Institute and you and your family can enjoy the summer sun safely while protecting your vision.
Sunglasses are more than just a great accessory
Sunglasses not only look great, they can help protect your eyes from harmful UV rays and reduce the chances of burning your corneas. Sunglasses should fit snugly around your eyes and offer protection on the side of the eyes as well. Keep in mind that sunlight is strongest mid-day, at higher altitudes, and when reflected off water or sand.
Choose sunglasses labeled “100% UV protection,” and only use glasses that block both UVA and UVB rays. It’s important to note that even if you wear UV blocking contact lenses, you still need to wear proper sunglasses to fully protect your eyes.
For maximum protection, wear a hat along with your sunglasses. Broad-brimmed hats are best.
Wear eye protection
Warm, sunny weather means it’s the perfect time for yardwork or to make a dent in your long list of home improvement projects. While doing work on your yard or home, it is extremely important to protect your eyes from dust, dirt and flying debris. Safety goggles can be purchased at home improvement stores, and do a better job of protecting your eyes than sunglasses.
Swim with goggles
Nothing says summer like a day at the beach or the pool. The chlorine in most swimming pools can be particularly irritating to the eyes, causing minor infections and dryness. Salt water from the ocean, rivers other natural bodies of water also contain contaminants that may be harmful to eyes. Wear swim goggles when you’re in the water to protect your eyes from irritants and floating particles that could damage your eyes.
Don’t forget the little ones
While it’s best to keep children out of direct sunlight during the middle of the day, they should wear sunglasses and hats to protect their eyes whenever they’re in the sun, and goggles when they’re swimming.
Eat right for your sight
Nutrition plays an important role in preventing conditions such as cataracts and macular degeneration. A healthy diet of summer foods like strawberries, tomatoes, avocadoes and peppers can help protect your eyes from many common eye conditions. Vitamins C, E and zinc have been shown to slow the aging process in eyes.
Drinking plenty of water can also help keep your eyes healthy. During summer months, it’s easier to become dehydrated, which can cause vision problems. Drink plenty of water to help keep your eyes healthy.
Year-round care
Eyes can be damaged by the sun – even through clouds and haze- any time of year so be sure to give your eyes the same protection year ‘round.
In addition to protecting your eyes in summer, annual visits for your eyes are important and beneficial for your overall health. A thorough eye exam – which is not the same as having a “vision test” – performed by an optometrist or ophthalmologist can detect potentially harmful diseases like diabetes, cardiovascular disease, thyroid disorders and cancers, vision disorders, and issues with the muscles in your eyes.
Georgia Eye Institute provides leading edge primary eye care, corrective eye surgery, ophthalmic care, and surgical eye care at 13 area offices. For more than 20 years the pioneering surgeons and staff at GEI have set new standards for outpatient cataract surgery and lens implantation, offers advanced retinal care for diabetic eye disease, LASIK laser vision correction, glaucoma management, treatment for macular degeneration and corneal disease, oculoplastic surgery, and optometry. For more information, visit gaeyeinstitute.com.
Diabetic Retinopathy FAQs
What is diabetic retinopathy?
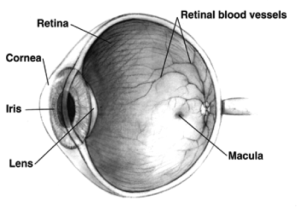
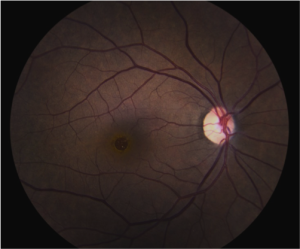
Long-standing diabetic disease (in Type I or Type II diabetics) can lead to changes in the back of the eye that can cause a decrease in vision. Specifically, high blood sugar causes damage to the small blood vessels in the retina (layer at the back of the eye that sense light). This damage leads to multiple changes to the retina, especially to the macula, which is responsible for central vision (Figure 1).
What are the different types?
There are two main types of diabetic retinopathy – “Non proliferative Diabetic Retinopathy” and “Proliferative Diabetic Retinopathy.” Proliferative indicates that new, abnormal blood vessels are growing inside the eye, which can lead to bleeding, retinal detachment, and high pressure (all leading to vision loss). Proliferative disease is more sever, but legal blindness can be caused by changes from non-proliferative disease.

Figure 1 – Normal Macula (the central part of the retina responsible for central vision)
Why do people lose vision from diabetic retinopathy?
Diabetes can lead to vision loss for many reasons, including:
- Swelling in the center part of the vision (Macular edema)
- Loss of blood flow to the center part of the vision (Macular ischemia)
- Bleeding into the central part of the eye (Vitreous hemorrhage)
- Detachment of the back layer of the eye from scar tissue (Retinal detachment)
How is it diagnosed?
The retina can be visualized during a routine eye exam after dilation of the pupil (Figure 3). Optical coherence tomography is a type of non-invasive imaging that allows your physician to view the macula and macular edema (if present) in cross-section (Figures 3 and 4). This is useful for following the disease over time.
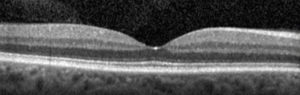
Cross sectional image (Optical Coherence Tomography, or OCT) of a normal macula. The “dip” in the center is the very center part of the vision, or the “fovea.” This is the “20/20? portion of the vision.
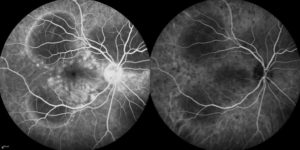
Figure 5. Photograph of the retina (angiogram) that shows loss of blood flow (dark areas).
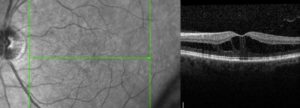
Figure 4. Cross sectional image (OCT) of a macula with diabetic macular edema. Notice the loss of the “dip” and black spaces in the retina. The retina is also thicker because of the swelling. This thickening leads to decreased vision.
How is it treated?
Treatment of diabetic retinopathy depends on the type of disease present. Good blood glucose and blood pressure control are essential in stabilizing disease.
Macular Edema
Edema that affects the center part of the vision is initially treated with medication that is injected into the eye (Figure 6). There are several medications available (Avastin, Lucentis, Eylea, Osurdex implant, steroid). For certain types of edema laser may be used. Laser can be used to destroy leaking blood vessels. A newer technology (micropulse laser) uses non-destructive energy to cause the macula to release factors that cause vessels to stop leaking.
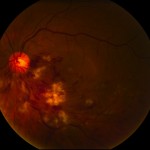
Figure 6. After the surface of the eye is anesthetized (numbed), a small amount of medication is injected into the middle of the eye (vitreous).
Proliferative Diabetic Retinopathy
Proliferative disease (especially if associated with bleeding [vitreous hemorrhage]) is generally treated with laser (panretinal photocoagulation). Laser is used to destroy sick tissue (areas in the back of the eye with loss of blood flow) – this causes abnormal blood vessels to shrink/resolve (Figure 7).
Vitreous Hemorrhage and Traction Retinal Detachment
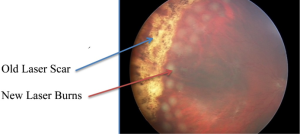
Figure 7. Photo of the retina shows vitreous hemorrhage covering the macula (center of vision) which blurs the vision. Laser scar can be seen peripheral to the blood. This patient required vitrectomy (surgery) to remove the blood.
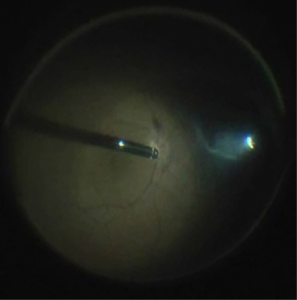
Proliferative disease that is untreated will lead to bleeding and retinal detachment. The blood itself will usually not harm the eye and will often resolve spontaneously. If the blood does not resolve or if there is retinal detachment that treats the macula (center part of the vision), surgery (vitrectomy) is necessary,. This surgery is performed in an operating room. Small instruments are introduced through micro-cannulas. One instrument provides light and the other instruments to remove blood and scar tissue and place additional laser (Figure 8).
When should a diabetic have a complete eye exam?
A type I diabetic should have their eyes examined within 3-5 years after diagnosis and yearly thereafter if no eye disease is found. A type II diabetic should have their eyes examined at the time of diagnosis and yearly thereafter if no eye disease is found. If diabetic retinopathy is present, follow-up and treatment depends on the severity of the disease or any other issues you may have.

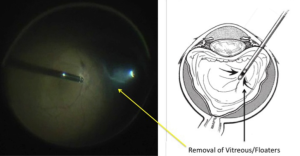
Removal of the vitreous from inside the eye using the “vitrector” (left side of picture). A small instrument (right side of picture) provides the light to see inside the eye. This is done under a microscope.
Cataract Awareness Month
June is Cataract Awareness Month
Cataracts are the leading cause of blindness in the United States, according to Prevent Blindness America, which declared June as Cataract Awareness Month. Cataracts affect more than 24 million Americans 40 and older. More than half of all Americans have cataracts by the time they are 80 years old, but cataracts can also appear in young adults or even newborns. Prevent Blindness America (PBA) estimates that by 2020, 30 million Americans will have cataracts. Unlike many other causes of vision loss, vision loss resulting from cataracts can be managed or significantly restored. There is no better time than Cataract Awareness Month to learn the symptoms and risk factors of cataracts, and to schedule an appointment with your eye care professional.
What Causes Cataracts?
There are several risk factors that may lead to cataracts, including:
- Heredity–family history of cataracts
- Inflammation of the eye
- Certain diseases such as diabetes or metabolic disorders, which can increase your risk of developing cataracts
- Intense heat or long-term exposure to UV rays from the sun
- German measles while pregnant can cause the newborn to be born with cataracts
- Long-term steroid use
- Eye injury, also known as traumatic cataracts
- Hypertension
- Smoking or alcohol use
- High myopia, or nearsightedness
- Medications such as statin medicines used to reduce cholesterol, or hormone replacement therapy
Cataracts may develop in one eye, particularly traumatic cataracts. More often, they develop in both lenses. Like myopia or astigmatism, they don’t always advance in the same way or at the same rate. One eye can have greater vision loss than the other as cataracts develop.
How does Cataracts Affect Vision?
The lens of the eye contains mostly water and protein. The protein in the eye is normally arranged in a way that keeps the lens clear, allowing light to pass through it. Cataracts occur when proteins in the lens of the eye begin to clump up.
The lens of the eye acts as a camera lens. It focuses light on the retina for clear vision. It also adjusts the eye’s focus, helping us to see things both close and far away.
There are several types of cataracts, and they are categorized by where they form and what causes them.
- A subcapsular cataract forms at the back of the lens. This type is more common in people with diabetes or those taking high doses of steroids. This form of cataract will interfere with reading and reduce your vision in bright light and can cause glare or halos around lights at night.
- A nuclear cataract forms in the nucleus (central zone) of the lens. These cataracts most often occur because of aging. This cataract will turn your lenses brown and interfere with your ability to detect color.
- A cortical cataract forms white, wedge-like opacities that start at the edge of the lens and work their way to the center. They look like wagon spokes and form in the lens cortex. This is the part of the lens that surrounds the central nucleus. These types of cataracts affect your peripheral vision and causes problems with glare.
Since cataracts tend to form over a long period of time, you may not know you have a cataract for years. If left undiagnosed, your vision may eventually acquire a brownish shade. Here, the cataract doesn’t affect your vision. As cataracts progresses, you may lose the ability to identify blues and purples. Your vision will start to dull or blur, and you will develop poor night vision, and halos may appear around lights, headlights, or lamplights. Having to change prescriptions in your eyeglasses or contacts regularly can also be a sign of a developing cataract.

How are Cataracts Detected?
A comprehensive eye exam includes testing for cataracts and other disorders of the eye such as macular degeneration and glaucoma.
You can expect:
- A review of your personal and family health history including any history of eye problems.
- A visual acuity test to determine how well you see at various distances.
- A dilated eye exam, where drops are placed in your eyes to dilate your pupils. Your retinas and optic nerves will be examined for signs of damage and other issues.
- Tonometry will measure the pressure inside the eyes. Numbing drops might be applied for this test.
If your doctor detects signs of a cataract, they might do additional testing to see whether your eyes are sensitive to light or if your peripheral vision (side vision) is affected.
If you are Diagnosed with Cataracts
There are several treatment options available for cataracts, depending on the severity. Your eye care professional will probably recommend new eyeglasses, brighter lighting, anti-glare sunglasses, or magnifying lenses. If these measures prove unsuccessful, the only option left is surgery. Some people can go years before needing surgery.
When the Treatment is Surgery
Traditional cataract surgery typically involves using a blade to remove the clouded lens and replacing it with an artificial one. It is usually only recommended when vision loss interferes with your daily activities, but it can also be recommended if it interferes with the eye care professional’s ability to examine or treat the rest of your eye. Laser cataract surgery provides a level of safety and comfort similar to bladeless LASIK where a femtosecond laser is used to make to make the incision.
Cataract surgery can slightly increase your risk of retinal detachment especially if you have other eye conditions which can also increase your risk. Talk with your eye care professional about the pros and cons of any options you are considering.
That said, cataract surgery is one of the most commonly performed surgeries, and is usually an outpatient procedure. More than 3 million Americans undergo cataract surgery every year, according to PBA. Nearly nine out of ten people who have cataract surgery regain very good vision, between 20/20 and 20/40.
It is important to speak with your doctor about vision issues you might be having, and to make informed decisions about the care and protection of your eyes. Your eye care professional should be able to sit down with you and discuss all your risk factors and help you weigh those against the benefits of the treatment options offered. If you are 65 or older, it’s important to get a complete eye exam every one or two years, even if you have no problems seeing. Schedule your appointment during Cataract Awareness Month and be proactive about your eye health.
6 Tips to Maintain Healthy Vision
6 Tips You Can Do Right Now to Maintain Healthy Vision
#1 – Wear Sunglasses
You probably know the sun can damage your skin… but did you realize the risk the sun poses on the health of your eyes? While sunglasses are a great aesthetic accessory, protection from UV Rays is ultimately what they’re used for.
Be careful to avoid these harmful side effects from the sun:
- Cataracts, which is when the lens of the eyes becomes cloudy, resulting in blurred vision. Approximately 20% of all cases are a result of UV exposure.
- Macular Degeneration happens when the retina is damaged and destroys central vision. This is the leading cause of blindness.
- Pterygium is a growth of tissue on the white part of the surface of your eye that affects the curve of your eyeball. The result is astigmatism.
When purchasing sunglasses look for something that blocks almost 100% of UVB and UVA radiation.
#2 – Quit Smoking
Did you know smoking can be harmful to your eyes? Sight -related problems are rarely discussed, so here are a few reasons that might help you kick the habit:
- Studies show that smokers are at three times the risk for developing AMD, and female smokers aged 80 plus are over 5.5 times likely to acquire AMD than those that don’t smoke and are the same age.
- Smoking doubles the risk of diabetes. Smoking is also a risk factor for progression of diabetic retinopathy, and hypertension.
- Smokers show higher rates of blindness and other issues in old age.
#3 – Annual Eye Exams Are Necessary
Recent studies have found that 25% of adults have not had their eyes checked in the last two years. Studies also show that 25% of all people are unaware that a simple eye exam can prevent blindness. If you’ve had laser vision surgery or are naturally blessed with good vision, it is still recommended that you have regular eye exams, preferably annually (after age 40).
“Vision tests” are not the same as having a complete eye exam. A thorough eye exam performed by an optometrist or ophthalmologist can detect potentially harmful diseases, vision disorders, and issues with the muscles in your eyes. If things begin to look blurry or you have trouble seeing objects far or near, this is an indication that you should have your eyes checked.
 #4 – Healthy Eating for Healthy Vision
#4 – Healthy Eating for Healthy Vision
There is a strong connection between food and one’s overall health. It has become apparent that having a healthy diet rich in vitamins and minerals provides long-term protection for your vision. Physicians tell us, “One of the best things you can do for your eyes is to eat a balanced diet high in fruits and vegetables, but also low in saturated fats and sugar.
#6 – Ensure the health of your Eyes by Washing Your Hands
The number of times you wash your hands daily can prevent the spread of infectious diseases, according to the Centers for Disease Control. By washing your hands frequently, you prevent the collection of dirt and germs that may be easily transferred to the eyes. This is caused by we touch this area subconsciously throughout the day. Not only will it reduce the chances of getting sick, it also helps control the spread of bacteria and viruses that are responsible for causing as-conjunctivitis (pinkeye) as well as corneal ulcers.
A great habit to practice is washing your hands before you eat or prepare food, before you treat injuries, before using any type of dispensing machine, and before you take out or put in contact lenses. An important instance where washing your hands should be your number one priority is before you get something in your eye or eyelash.
Some quick facts to digest when it comes to the protection of your eyes via washing your hands:
- Half of all people fail to wash their hands after sneezing or coughing.
- Over half of all men and almost one fourth of women doesn’t wash their hands after using restroom facilities.
- Over one third of all people don’t think it is necessary to wash their hands before a meal.
- Left-handed people tend to wash their right hand more thoroughly than they’re left and conversely for right handed people.
We hope these tips help you in your quest for top-notch vision! For more information please visit our Homepage.
Cataract Newsletter
Cataract Surgery Risks and Benefits
Cataract surgery has changed over the past 20 years from large incisions with long recovery times to our current surgery with a 2.4mm incision, self sealing wound, and possible expectations of refractive benefits where glasses are not required for distance nor near. Some of the greatest difficulties with cataract surgery involve managing reasonable expectations.
This letter will review cataract surgery and its risks and benefits. It will focus on the new refractive options that are available because of new lens designs. Lastly, it will review unexpected benefits about glaucoma.
Cataract surgery involves the removal of a cloudy lens from the center of the eye and its replacement with a thin plastic lens that is designed to focus the light on the retina. The normal lens is optically clear but as we age, and occasionally in association trauma or illness, the lens becomes cloudy and discolored. It is no longer able to focus the light but rather causes the light to amplify or scatter in a random manner, what you might describe as glare or blurred vision. If these changes interfere with your daily activities and quality of life, it is reasonable to consider surgery. Your doctor will also consider other factors, beyond the scope of this letter, when considering your cataract.
While cataract surgery is one of the most successful and predictable surgeries, risks are still present. To each patient it remains a major surgery as there is the potential for vision loss and rarely actual loss of the eye from infection, bleeding or retinal detachment.
The excitement of cataract surgery comes from the refinements in instruments that allow a very small self sealing wound and the precise calculation of a monofocal lens implant that minimizes the need for glasses after surgery. Often, the residual refractive error, or need for glasses, is not significant and the patient is content with only reading glasses.
The special lens is also available to treat most astigmatism. These toric lenses are aligned with your eye to treat the moderate corneal irregular curvature that is not treated by a standard lens. The higher level of premium lens implant is a multifocal lens that is designed to minimize the need for distance and near vision glasses. There are multiple brands that utilize different technologies, but the goal is to have some light focused for near and some for far. This may limit contrast sensitivity and can be associated with a glare but for many patients, the benefits far exceed these issues. Not every patient is a candidate for the toric or the multifocal implant and for that reason, Medicare allows an out of pocket charge for the extra evaluation and services. Patients with dry eyes or other surface abnormalities do not tolerate these lenses well, and some consider macular degeneration to be a relative contraindication. Your doctor will take these factors into consideration if you are considering a premium lens implant.
Recent studies have highlighted other benefits of cataract surgery.
 The Ocular Hypertension Treatment Study reported on the benefits of cataract surgery in patients with ocular hypertension in September 2012. The report had a better design and confirmed what other studies had reported, a reduction in postoperative intraocular pressure. There was an average 16.5% reduction in IOP and there was a greater reduction in eyes with the highest preoperative pressure. A lower intraocular pressure limits the potential for glaucoma damage and in some patients may make glaucoma drop therapy no longer necessary. This can be a considerable financial saving given the price of glaucoma medications.
The Ocular Hypertension Treatment Study reported on the benefits of cataract surgery in patients with ocular hypertension in September 2012. The report had a better design and confirmed what other studies had reported, a reduction in postoperative intraocular pressure. There was an average 16.5% reduction in IOP and there was a greater reduction in eyes with the highest preoperative pressure. A lower intraocular pressure limits the potential for glaucoma damage and in some patients may make glaucoma drop therapy no longer necessary. This can be a considerable financial saving given the price of glaucoma medications.
In July 2012, a new study published in The Journal of the American Medical Association examined the incidence of hip fractures in the year after cataract surgery. The study showed 16% fewer hip fractures in the year after surgery. Interestingly, the patients between the ages of 65 and 69 had a slightly higher rate of hip fracture but the patients ages 80 to 84 experienced a 28% reduction in hip fractures compared to those Medicare beneficiaries who did not have cataract surgery.
Other studies have shown benefits in mental health and overall quality of life after cataract surgery. It is a very exciting time in ophthalmology and cataract care. It is amazing to think of the distance we have covered in the last 20 years. While all surgeries carry some risk, there is a lot more to be excited about than feared when you are told, “ You have cataracts and we need to consider surgery to make you see better.”
For more information please visit our Home Page.
Flashers, Floaters and Retinal Detachment
What are flashers and floaters? What causes them?
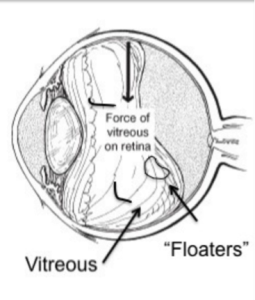
The center of the eye is filled with a clear gel called vitreous. When we are born, the vitreous in both eyes is completely clear and stuck down everywhere to the inside surface of the eye (including the retina). As we get older the gel clumps together, these cast shadows on the retina (light sending part of the eye) causing the occasional floaters we see.
After several decades (usually after age 50) the gel liquefies and starts to separate from the back of the eye. This is called posterior vitreous separation, or detachment. When this occurs a larger floater can be seen. People sometimes describe this as a circle, a cobweb, a spider, etc. (Figure 1).
 As the separation progresses (usually over 4-6 weeks) the gel can tug on the retina (back of the eye). This causes flashes of lights. Though the flashes do not cause damage, a flash could indicated that the gel is pulling especially hard increasing risk of a tear in the retina.
As the separation progresses (usually over 4-6 weeks) the gel can tug on the retina (back of the eye). This causes flashes of lights. Though the flashes do not cause damage, a flash could indicated that the gel is pulling especially hard increasing risk of a tear in the retina.
The appearance of flashes and floaters may be alarming, especially if they develop suddenly. You should contact your eye doctor right away if you suddenly develop new flashes or floaters.
Are floaters ever serious?
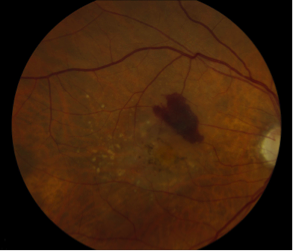
The retina can tear if the shrinking vitreous gel pulls away from the wall of the eye. This sometimes causes a small amount of bleeding in the eye that may appear as new floaters. A torn retina (Figure 2) is always a problem, since it can lead to a retinal detachment. You should call your eye doctor as soon as possible if:
- Even one new floater appears suddenly
- Lots of “pepper spots” in your vision
- You see sudden flashes of light
- You notice loss of any peripheral (side) vision
How are your eyes examined for flashes and/or floaters?
When an ophthalmologist examines your eyes, your pupils will be dilated with eye drops. During this examination, your ophthalmologist will carefully observe your retina and vitreous using a bright light. Evaluation for retinal tears usually requires a technique called scleral depression, for which your ophthalmologist will use an instrument to gently press on your eyelids. This office examination is done with minimal discomfort. Because your eyes have been dilated, you may need to make arrangements for someone to drive you home afterwards.
Floaters and flashes of light become more common as we grow older. While not all floaters and flashes are serious, you should always have a medical eye examination by an ophthalmologist to make sure there has been no damage to your retina.
What can be done about floaters?
Floaters can get in the way of clear vision, which may be quite annoying, especially if you are trying to read. Though most floaters will always be there, people usually notice less over time. Floaters can be surgically removed (with surgery called vitrectomy – Figure 3), but this is not performed routinely as most people have minimal symptoms after a couple of months. Even if you have had some floaters for years, you should have an eye examination immediately if you notice new ones.
{kind=link}
What is retinal detachment?
The retina is the sensory tissue that lines the back wall of the eye. It can be described as the wallpaper of the back of your eye. A retinal detachment occurs when the retina is separated from the inside of your eye and can no longer transmit images properly through the optic nerve to the brain. The center of the retina is the macula. If the macula is involved in the detachment, the vision is often extremely blurred. If the macula is not involved in the area of detachment, there may be some loss of peripheral vision.
Is a retinal detachment serious?
Yes. A retinal detachment is a very serious problem that will almost always lead to blindness if not treated.
What causes retinal detachment?
As described above, in some cases vitreous separation can cause a tear (or tears) in the retina. As time passes, fluid from the center of the eye will pass through the tear and begin accumulating beneath the retina, causing a retinal detachment. There are some conditions that increase the likelihood of developing a retinal detachment. These include:
- Myopia (nearsightedness)
- Traumatic Injury
- A history of retinal detachment in either eye
- Family history of retinal detachment
What are the symptoms of retinal detachment?
- A new floater or several floaters can be hundreds) that appear suddenly
- Sudden flashes of light in the eye
- Seeing “cobwebs” or hairs in the field of vision
- Impression of a curtain or veil coming down over vision (loss of peripheral, and then central, vision)
- Blurred vision
- Pain is not a symptom of a detached retina
How is retinal detachment repaired?
A retinal detachment can be repaired in several different ways. The surgery chosen depends on the age of the patient, the type of retinal detachment, whether the patient has had cataract surgery or not, surgeon preference, and other factors. The four general categories of retinal detachment are:
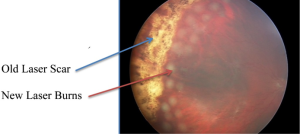
Figure 5
- Laser barricade (Figure 5) – does not fix the detachment but prevents it from spreading; can be done in the office).
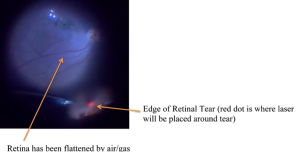
- Pneumatic Retinopexy – a combination of treating the tear with cryotherapy (freezing treatment) or laser and the use of a gas bubble injected into the eye to help the eye get rid of the fluid. Figure 6 shows the injection of a gas bubble that will cover the tear in the retina. This prevents fluid from getting behind the retina and allows the body to absorb the fluid and flatten the retina.
- Scleral Buckle – a scleral buckle involves first treating the tear in the retina with cryotherapy (freezing treatment) and then placing a silicone band under the muscles around the eye to support the tear. The fluids can be drained from under the retina or a gas bubble can be injected into the eye similar to pneumatic retinopexy.
- Vitrectomy – vitrectomy involves the removal of the vitreous (floaters) from the eye using small instruments (Figure 3). This removes all the traction (pulling) on the retinal tear(s) and detachment. The vitreous space is then filled with a long-lasting gas bubble that keeps the retina flat until the tears heal. Laser is then used to seal the tear(s) (Figure 8).
Figure 8
Sometimes both a scleral buckle procedure and a vitrectomy are used together to fix complex retinal detachments.
All diagrams from Ryan SJ, Retina. 4th ed. www.retinatext.com, Elsevier; 2006
See Your Eye Doctor Every Year
Why you should see an eye doctor annually
Your vision is a critical part of your overall health. When going in your regular annual physical checkup, it is important to also make sure that you have your vision checked as well. During an eye exam, your physician will check for signs of glaucoma, age-related macular degeneration, cataracts and diabetic retinopathy, among other diseases. So what is part of a traditional eye exam?
Eye Exam
The doctor will perform these typical eye tests as part of your annual exam. The first is the eye muscle movement test, which is meant to make sure that your eyes are aligning normally. Part of the test includes having your doctor ask you to track targets in various directions, then they will observe how your eye moves and note any areas of potential concern. If there are areas of concern, your doctor will prescribe treatments to deal with those concerns.
 Cover Test
Cover Test
The cover test is a check of how well your eyes are working in concert with each other. As you stare at a designated target in the distance, the doctor will cover and uncover your eyes one at a time. This will allow them to observe the movements of your eyes, watching to see if one of the eyes turns away from the target. This test can be repeated with the target close by as well.
External Test
During the external exam and pupillary reactions will test your pupils ‘reactions to both light and other objects at close distances. The doctor will also examine the exterior of the eye, looking for any changes in the condition of the white area of the eye and the overall position of the eyelids. If you continue to have a regular annual exam, then your doctor can track any changes over time and address them right away.
Visual Acuity Test
The visual acuity test requires you to sit in front of an eye chart, with letters that get gradually smaller as you read down the lines. You may be required to cover one eye or the other as part of this test. Depending on how good your vision is, you may be able to read the whole chart or be stuck part way down.
If you have difficulties with this chart, then you may be required to get a prescription for glasses or contacts to correct your vision issues. This will mean that you need to have a refraction test to determine your exact lens prescription. Additionally, you may need to have a glaucoma test to check the fluid pressure in your eyes falls within the normal range. The test is painless and usually takes just a few minutes to perform.
There are a few other tests that are included in a typical eye exam, but all these check the health of your eyes and their various parts. These tests are all geared to locating any potential issues with your eyes, but also how they can be indicative of other diseases or potential issues within your body as a whole. Be sure to have your eyes checked annually as part of an overall healthy lifestyle.
Macular Hole FAQs
What is Macular Hole?
A macular hole is a small full-thickness defect in macula, the most important region of your retina. The macula is the center of the retina, which is the light sensing part of the back of the eye. Formation of the hole causes loss of central vision (reading, driving, recognizing faces is affected).
What types of symptoms do patients with Macular Hole have?
Symptoms vary based on the size of the hole. The most typical symptoms are:
- Distortion of vision (called metamorphopsia) – letters look crooked
- Blurred vision or loss of visual acuity
- Dark spot at center of vision (central scotoma) – patients describe missing letters in words when looking right at the word. These dark spots are different than floaters as they do not move around.
- Patient often first notices the vision loss when they cover up the unaffected/good eye.
What causes a Macular Hole?
The most common cause of a macular hole is a posterior vitreous degeneration. This is when the vitreous gel that fills the center of the eye liquefies and separates from the back surface of the inside of the eye (the retina). This results in traction/pulling in the central macula. If there is enough traction a hole forms.
Direct ocular trauma by a blunt force, like a tennis ball, can cause macular holes to form as well. This group of patients is more likely to have spontaneous closure without surgery.
Who is at risk?
Most patients that develop macular problems are in their 60s or 70s and women are more commonly affected. Most people will experience vitreous degeneration, but macular hole is not very common. It is not associated with any systemic disease.
 How are they diagnosed?
How are they diagnosed?
The macula can be visualized during a routine eye exam after dilation of the pupil. Optical coherence tomography is a type of non-invasive imaging that allows your physician to view the macula and macular hole (if present) in cross-section. This allows your physician to measure the exact size of the hole and study the anatomy. This is useful for knowing the likelihood of closure with surgery.
How are they treated?
Small holes will often spontaneously close/heal without treatment. In some cases medication (Jetrea) can be injected into the eye that will release traction on the hole and allow it to close, however there are a very few eyes that are candidates for this medication. Most macular holes are treated with surgery.
Surgery consists of vitrectomy to remove the vitreous gel (floaters) from the middle of the eye (Figure 6). Micro-forceps are then used to gently peel the membrane from the retinal surface from around the hole (Figure 7).
What is the vision like after surgery?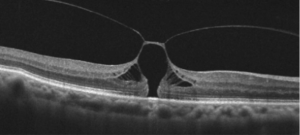
The vision is poor the day after surgery due to the gas bubble. Vision through gas is distorted and will remain so until the bubble resolves. There are usually position requirements after surgery to ensure the bubble is correctly positioned against the hole (each surgeon has their own post-operative position requirements based on their specific surgical technique). Historically, the patient was required to position face down for 14 days but currently close to 100% anatomical success can be achieved without face down positioning. The only requirement is that the patient not sleep on his/her back but to favor the opposite cheek being on the pillow.
Vision will improve after the gas bubble dissolves (this takes several weeks and timing depends on the type of gas used). Visual improvement can continue to occur for 9-12 months after successful surgery. If it has not already been removed, the cataract (cloudy lens of the eye) will worsen with this type of surgery, and this will cause worsening vision. Many times a combined approach is used and the cataract is removed at the same time as surgery for the macular hole.
Healing and approximation of the edges of the hole is out of the control of the surgeon. If the hole was small, the margins may come back perfectly and the vision returns to near normal. However, the tissues may not meet perfectly and there can be some residual distortion and blurred vision even if the hole is closed. There can be a persisting central dead spot in the vision if the central defect is filled in with scar tissue and the edges did not meet. This is most common in longstanding holes and larger holes.
 What are the restrictions after surgery? What are the risks of surgery?
What are the restrictions after surgery? What are the risks of surgery?
Restrictions in the postoperative period are most commonly related to the gas and the secondary poor vision. You cannot fly or travel to the mountains with an eye filled with gas. Patients should not drive or participate in activities that require depth perception and may result in injury.
Any intraocular surgery involving vitrectomy has a low risk of infection, bleeding, retinal detachment, and other complications, which can all lead to permanent vision loss. Risks, benefits, and alternatives to surgery should be discussed with your eye surgeon prior to proceeding with vitrectomy for macular hole.
Patient Portal
Patient Portal – Fast, Easy and Secure Communication
The Patient Portal is a website through which you may communicate with our office. Registered patients would have secured and confidential access to the website and may:
- Ask a question
- Receive a clinical summary of your office visit
- Receive results, education material and information online
- Request an appointment
- Request a medication refill
Why are we using the Patient Portal?
Implementing a patient portal bridges the gap between you and your provider and provides more efficient communication.
Sign Me Up!
To create an account in the Patient Portal, call us at 912-354-4800 or visit us and our expert staff can help you. We will create a NextMD account for you and give you a personal enrollment token (an 8-digit number used to sign in). Once we create your account, you will receive an email with instructions on how to enroll in the Patient Portal.
 It’s Fast!
It’s Fast!
The Patient Portal provides instant, direct access to our providers and staff, providing a more streamlined health care experience. You can send and receive messages to staff and providers regarding your health care needs. You can request to renew medications online which will speed up the prescription process. Patient education, diagnostic testing results and a clinical summary of your visit will be sent to you so you can get on with your day.
It’s Easy!
The Patient Portal will allow you to request and manage your appointments at your convenience, from the comfort of your home or office. You can submit a request for an appointment or a medication refill 24 hours a day, 7 days a week. Once submitted, requests will generally be handled within 1-2 business days, excluding holidays, and weekends. If you have a non-urgent question, you can send us a message through the Patient Portal and we will answer the question as soon as possible. No more holding on the phone lines or waiting for a phone call back!
It’s Safe!
Our patients’ privacy is our number one concern. The Patient Portal is HIPAA compliant and gives secure access to each user so you can feel safe when using it. Each patient creates their own unique password and is asked a security question each time they login for maximum safety. No medical or personal information will be sent to you through your personal e-mail account.
Call us today at 912-354-4800 or visit us and our expert staff can help you!
Are e-readers bad for your eyes?
Are e-readers bad for your eyes?
If you’re a bookworm, you’re well aware there are plenty of ways to get your fix these days , with everything from paperbacks to Kindles.
Reading on a device, like a kindle or an iPad, has a very different effect on your eyes than does a good, old-fashioned book. But should you avoid them? We talked to an ophthalmologist to find out.
Folks usually feel pretty strongly about this one way or the other. Some love the feel of a book in their hands, while others swear by e-readers. Which one is the better for your eyes? The answer is not so easy. The two have more commonalities than differences.
Dr. Elizabeth Miller with the Georgia Eye Institute says overall, the words you see in a book aren’t much different than what you see in the electronic form, but when it comes to user preference…
“From the standpoint of user friendly, the eBooks, Kindles, iPads, and Nooks are much easier,” she said.
She says it is important though, to differentiate between the types of e-readers out there.
“E-Books are much more like real books. If you have a Nook or Kindle, it’s much more like a real book. Light is reflected. If you have a computer or iPad or Phone, those lights are projected; little pixels that all come together. Studies show when you use that type of device, it’s more tiring and stressful for your eyes,” Dr. Miller said.
 She says that eye stress is all too common, in the form of…
She says that eye stress is all too common, in the form of…
“I see dry-eye the most in my office. Studies show when you sit down to your computer, iPad or Nook, you blink one-quarter of the time you normally would, so your eyes get dried out.”
Does that sound familiar? If you’re wondering what you can do to prevent this, here’s some advice.
“If you read for 20 minutes, take a 20-second break from reading, and look at something 20 feet away, and if you’re worried about the long-term effects of e-readers on your eyes, Dr. Miller says, don’t be!
“Won’t cause cataracts or glaucoma earlier. Will cause surface issues, in terms of dryness or irritation. I wouldn’t suggest staying away from any of those. Choose your battles.”
Dr. Miller says if you start getting intermittent blurriness, discomfort or tearing while reading, visit your doctor right away.
WTOC-TV: Watch The Full Interview – Click Here
Original Source and Copyright 2016 WTOC. All rights reserved.